-Abortion (Miscarriage)-

-Spontaneous abortion or miscarriage is pregnancy loss before 20 weeks of gestation
-The frequency of spontaneous abortion decreases with increasing gestational age
-Eighty percent of spontaneous abortions occur in the first 12 weeks of gestation
-The overall risk of spontaneous abortion after 15 weeks is low (about 0.6 percent)
-Major risk factors for spontaneous abortion include advance maternal age, previous spontaneous abortion, and maternal smoking
-Some studies have shown increase risk of spontaneous abortion with increasing gravity
-Substances and medications that can cause spontaneous abortion include: smoking, alcohol, cocaine, and NSAIDS
-Other factors that may influence spontaneous abortion include: low plasma folate levels, extremes of mothers weight, fever during pregnancy, and celiac disease
-The etiology of spontaneous abortion is most caused by chromosomal abnormalities or exposure to teratogens
-Pregnancy loss may be to septum uterus, leiomyoma, intrauterine adhesion. Material infections such as listeria, toxoplasmosis, parvovirus B19, rubella, HSV, CMV, or lymphocytic choriomenigitis virus can result in abortion due to fetal or placental infection
-Clinically presents with vaginal bleeding and pelvic pain.
-Spontaneous abortion may be detected incidentally by absence of fetal cardiac activity on hand held doppler or by pelvic ultrasound
-Pelvic Exam should be performed to look to make sure the uterus is the source of the bleeding rather than a vaginal lesion
-Subchorionic hemorrhage or hematoma is a risk for spontaneous abortion
-Quantitative HCG and ABORh should be drawn when spontaneous miscarriage or suspected. Women who are Rh negative need to get Rhogam.
-Diagnosis of spontaneous abortion is made usually by pelvic ultrasound
-Differential diagnosis of bleeding or pain in early pregnancy includes: physiologic, ectopic pregnancy, gestational trophoblastic disease, subchorionic hematoma, cervical, vaginal or uterine pathology
-Threatened miscarriage is bleeding and pain but cervical os is closed and the diagnostic criteria for spontaneous miscarriage is not met.
-Missed abortion is a spontaneous abortion in a patient with or without symptoms having a closed cervical os.
-Incomplete abortion is when vaginal bleeding and or pain are present, the cervix is dilated and products of conception are found within the cervical canal on examination
-Complete abortion is when products of conception are entirely out of the cervix and uterus
-The conventional treatment of first or early second trimester failed pregnancy is dilation and curettage is perfumed to prevent potential hemorrhagic or infectious complications
-Misoprostol, a prostaglandin E1 analog, is available when women who want to avoid surgery and where surgical intervention is not practical
-Abruptio Placentae-
Placental abruption is bleeding at the decidual placental interface that causes partial or total placental detachment prior to delivery of the fetus
-The diagnosis of placental abruption is typically reserved for women over 20 weeks
-Placental abruption can cause significant material and perinatal morbidity and perinatal mortality
-The perinatal death rate of placental abruption is about 12 percent
-Major risk factors for placental abruption are: abdominal trauma, cocaine and other drug use, polyhydraminos, chronic hypertension, preclampsia, pregnancy induced hypertension, premature rupture of membranes, chorioamnioitis, increasing maternal age, parity, smoking during pregnancy, and male sex of the infant
-Retroplacental hematoma is the classic ultrasound finding with placental abruption
-Classically women over 20 weeks present with acute onset of mild to moderate vaginal bleeding and abdominal and/or back pain
-All patients with acute placental abruption need to be monitored and undergo continuous fetal heart rate assessment until their status is clear
-Want to have large bore IV access and to keep mother warm with SpO2 greater than 95%
-Lab workup should include CBC, Blood Type and Rh, and Coagulation studies. The anesthesia team should be notified
-Indications for delivery with placental abruption are as below:
1. Delivery non severe abruption over 36 weeks, or severe abruption at any age
2. Non Severe Abruption between 34-36 weeks
-Non Severe Abruption less than 34 weeks should be delivery when the mother is stable and tests of fetal well being are reassuring
-Cesarean Section-

- C-Sections have two major different techniques: transverse incision, and low vertical and classical incision
-Transverse incision is recommended for most C-Sections. It employs a transverse incision along the lower uterine segment. There is less blood loss, less bladder dissection, easier reapproximation and a lower risk of rupture with subsequent pregnancies
-A Low Vertical incision is perfumed in the lower uterine segment and appears to be sat strong as the low transverse incision
-A vertical incision that extends into the upper uterine segment is a classical incision. This is rarely performed at or near term because subsequent pregnancies it is associated with higher frequency of uterine dehiscence or rupture
-Indications for C-Section:
1. Failure to Progress
2. Non Reassuring Fetal Status
3. Fetal Malpresentation
4. Abnormal Placenta
5. Multiple Gestation
6. Maternal Infection
7. Fetal Bleeding Diathesis
8. Cord Prolapse
9. Suspected Macrosomia
10. Uterine Rupture
11. Mechanical Obstruction to vaginal birth
-Dystocia-

-A shoulder dystocia complicates a vaginal delivery when after delivery the fetal head, additional maneuvers beyond gentle traction are needed to enable delivery of fetal shoulders
-The goal of management of shoulder dystocia is to prevent asphyxia and permanent Erb's palsy, while avoiding physical injury
-Shoulder dystocia is a subjective diagnosis made during delivery
-Most interventions are intended to disimpact the anterior shoulder behind the symphysis pubis by rotating the fetal trunk or delivering the posterior arm and shoulder
-Ectopic Pregnancy-

-Ectopic pregnancy occurs when the developing blastocyst become implanted at another site other than the endometrium of the uterus
-Most common extrauterine location is the fallopian tube (98% of ectopic pregnancies)
-Hemorrhage from ectopic pregnancy is still the leading cause of maternal related death in the first trimester
-The guiding principle has evolved to attempts to save the tube rather than salpingectomy
-Risk factors for ectopic pregnancy include: previous ectopic pregnancy, tubal pathology or surgery of the tube, in utero exposure to DES, previous genital infections, IUD, multiple sexual partners, smoking, IVF, vaginal douching, age less than 18
-A Heterotopic Pregnancy is a combination intrauterine pregnancy and a concurrent pregnancy at an ectopic location
-Classic symptoms of ectopic pregnancy are abdominal pain, amenorrhea, and vaginal bleeding
-Clinical manifestations typically appear 6-8 weeks after the last normal period
-Physical exam findings may include adenexa tenderness, cervical motion tenderness, and abdominal tenderness
-Lab work up includes CBC, quantitative HCG, blood type and screen
-A serum HCG level is greater than 1500, a IUP should be visualized at most institutions. A gestational sac has been identified as low as 800.
-If the quantitative HCG is too low, OB follow up should be arranged in 48 hours with repeat ultrasound if increases. Differential diagnosis at this point is early IUP not seen, early ectopic, or missed abortion
-If the transvaginal ultrasound does not reveal an intrauterine pregnancy, and shows a complex adenexa mass, this is an ectopic pregnancy until proven otherwise
-Methotrexate can be used in hemodynamically stable ectopic pregnancies that are willing to comply with post treatment follow up if there is a beta HCG less than 5000 and no fetal activity.
-Women with ectopic pregnancy that should be treated surgically include: hemodynamically unstable, signs of impending or ongoing ectopic mass, clinically important abnormalities in baseline hematologic labs, immunodeficiency, active pulmonary disease or peptic ulcer disease, hypersensitivity to methotrexate, breastfeeding, coexistent viable intrauterine pregnancy, non compliant patients, and patients that do not have timely access to a medical institution
-Fetal Distress-

-Normal fetal heart rate is 110-160
-Acceleration is an abrupt increase in the fetal heart rate. Before 32 weeks accelerations should last greater than 10 seconds and peak over 10 bpm. After 32 weeks gestation, accelerations should last greater than 15 seconds and peak 15 bpm above baseline.
-Late Deceleration is a gradual decrease and return to the baseline associated with a uterine contraction. . The deceleration is delayed in timing, with the nadir of the deceleration occurring after the peak of the contraction
-Early Deceleration-a gradual decrease and return to the baseline fetal heart rate associated with a uterine contraction. The deceleration is delayed in timing with the nadir of the declaration occurring at the same time of the peak of the contraction.
-Variable Deceleration-an abrupt decrease in the fetal heart rate from baseline. The decrease is greater than 15 bpm and lasts greater than 15 seconds and less than 2 minutes from the onset of rerun to baseline. The onset, depth, and duration of variable declarations commonly vary with successive uterine contractions
-Prolonged Deceleration- a decrease in the fetal heart rate below baseline. The decrease is greater than 15 seconds, lasts at least 2 minutes but less than 10 minutes from onset to return to baseline. A prolonged deceleration for over 10 minutes is considered a change from baseline.
Non Stress Test- usually performed past 26-28 weeks when neurological development enables fetal accelerations. Reactive tests are two accelerations occurring in a 20 minute period. Non reactive stress tests does not show accelerations over a 40 minute period
-Gestational Diabetes-

-Women are screened for diabetes at 24-28 weeks gestation.
-Complications of gestational diabetes include:
1. Large for Gestational Age and Macrosomia
2. Preclampsia
3. Polyhydraminos
4. Stillbirth
5. Neonatal morbidity
-Long term can affect offspring causes obesity, development of metabolic syndrome, and impaired glucose tolerance. Can also lead to maternal type 2 diabetes and vascular related complications
-Treatment includes counseling, monitoring, nutritional therapy, insulin, and oral anti hyperglycemic drugs if needed
-If estimated fetal weight is greater than 4500 grams offer a C-Section, if less than 4500 grams can offer trial of labor if appropriate
-During labor periodic assessment of material glucose is needed and needs to be treated. The goal of treatment is to reduce the risk of neonatal hypoglycemia
-After delivery, women with gestational diabetes should be able to resume a normal diet after the placental hormones dissipate.
-Breastfeeding is encouraged after delivery
-Normal values are Fasting Glucose Less than 95
-1 hour post prandial less than 140, and 2 hour post prandial less than 120
-Gestational Trophoblastic Disease-
-Gestational Trophoblastic Disease (GTD) is a proliferative disorder of the trophoblastic cells characterized by interrelated lesions arising from the trophoblastic epithelium of the placenta
-All forms of GTD are characterized by tumor marker beta HCG
-Several types of GTD-
1. Hydatidiform Mole (complete or partial)
2. Persistent/Invasive Gestational Trophoblastic Neoplasia
3. Choriocarcinoma
4. Placental Site Trophoblastic Tumors
-Hydatidiform Moles are noninvasive. They make up 90% of all GTD. They are a result of aberrant fertilization event that leads to proliferative process
-Malignant GTD can develop from a molar pregnancy or can arise after any gestational experience
-Risk factors are the very old and very young and history of previous GTD
-About 40% of complete moles are associated with HCG greater than 100,000
-Complete mole include the absence of fetus or embryo and no amniotic fluid, central heterogenous mass with numbers discrete anechoic spaces
-After treatment of molar pregnancy HCG levels should be monitored serially to make sure returns to baseline
-GTD can be treated with single agent such as chemotherapy, or combination of chemotherapy and surgery. Depends on staging
-Hypertension Disorders in Pregnancy-

-Four Types of Hypertensive Disorders in Pregnancy-
1. Gestational Hypertension-elevated BP first detected after 20 weeks gestation in the absence of protein in the urine or other diagnostic features of preclampsia
2. Preclampsia/Eclampsia- Preclampsia is a syndrome of new onset hypertension and either proteinuria or end organ dysfunction most often after 20 weeks in a previously normotensive patient. Eclampsia is diagnosed when seizes occur
3. Chronic Hypertension-is defined as systolic pressure over 140 or diastolic over 90, that precedes pregnancy and is present before the 20th week of pregnancy, or persists for over 12 weeks post partum
4. Preclampsia superimposed on chronic hypertension-when a woman with previous hypertension is diagnosed with worsening hypertension with not onset proteinuria and other features of preclampsia such as elevated liver enzymes or low platelets
-Severe hypertension (Greater than 160/110) has been well established as benefits of treated for maternal reduction of stroke
-Mild to moderate hypertension may not be beneficial to treat short term. Exposes fetal to potentially harmful medications and can inhibit fetal growth
-Treatment options such as methyldopa and labetolol are considered safe and effective
-Nifedipine appears to be safe and effective in pregnancy
-Hydralazine has been used extensively in the treatment of severe hypertension and preclampsia
-ACE inhibitors, ARB's, and Nitroprusside should be avoided in pregnancy
-Diuretics can reduce milk volume post partum
-With preclampsia we treat blood pressures that are consistently over 150/100
-Baseline labs include, BMP, glucose, urine, and quantitative analysis of urine protein
-Ultimately the "cure" for preclampsia is delivery
-Multiple Gestation-

-Multiples can be monozygotic or dizygotic. Dizygotic multiples result from the fertilization of multiple follicles. Monozygotic multiples divide from a single ovum
-The plasma concentration of FSH being high seems to correlate with rates of dizygotic births
-Dizygotic twins have two placentas
-The risk for preterm labor is higher in multiple pregnancies than singletons
-The growth of twins is not significant from singletons from the first and second trimester. There have been some studies that have shown some slower growth after 30 weeks gestation with multiples compared to singletons
-Higher rates of intrauterine growth restriction (IUGR) contribute to adverse outcomes of twin births
-Small for gestational age and discordant growth are complications of twin births
-Complications of multiple gestations include: neurological developmental disorders, twin twin transfusion syndrome, and congenital abnormalities.
-Conjoined twins are a complication of monozygotic twins
-Placental Previa-
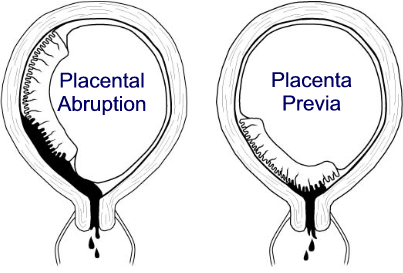
-Placenta previa is the presence of placental tissue that extends over or lies proximate to the internal cervical os.
-Placental previa should be suspected with painless bleeding beyond 20 weeks gestation
-Possible risk factors include: previous C-Section, multiple gestations, multiparity, advanced material age, infertility treatment, previous abortion, previous intrauterine surgical procedure, material smoking, maternal cocaine use, male fetus, and non white race.
-Pathogenesis is unknown of placental previa
-Placental bleeding is thought to occur when gradual changes in the cervix and the lower uterine segment apply shearing forces to the inelastic placental attachment site resulting in partial detachment
-Ten to twenty percent of patients with placental previa will present with uterine contractions and bleeding which is similar to the presentation of placental abruption
-Complications of placental previa include:
1. Placenta Accreta
2. Preterm labor and premature rupture of membranes
3. Malpresentation
4. Intrauterine growth restriction
5. Vasa previa and velamentous umbilical cord
6. Congenital abnormalities
7. Amniotic fluid embolism
-Diagnosis is confirmed with ultrasound
-Pelvic rest until cleared by OB
-Will need a C-Section if continues until term
-Post Partum Hemorrhage-

-Postpartum hemorrhage is an obstetrical emergency that can follow a vaginal or c-section
delivery
-Primary Postpartum Hemorrhage occurs in the first 24 hours after delivery
-Secondary Postpartum Hemorrhage occurs 24 hours to 12 weeks after surgery
-Post partum hemorrhage is excessive bleeding that makes the patient symptomatic and results in signs of hypovolemia
-Hemorrhage may not necessarily vaginal can be internal when related to broad ligament or vaginal hematoma
-Postpartum hemorrhage can result from defective myometrial contraction (atony), defective decidual hemostasis, trauma, bleeding diathesis, or thrombocytopenia
-Risk factors include: retained placenta, failure to progress, placenta accreta, lacerations, instrumental delivery, large for gestational age newborn, hypertensive disorders, induction of labor, or augmentation of labor
-Timely management includes accurate diagnosis and initiation of appropriate interventions: drugs surgery, and referral
-Adequate IV access for massive transfusion, active management with third stage of labor with oxytocin, misporstol may be needed.
-Premature Rupture of Membranes-

-Premature Rupture of Membranes (PROM) refers to rupture of membranes before the onset of uterine contractions. It is considered Preterm Premature Rupture of Membranes (PPROM) if it occurs before 37 weeks gestation
-Risk factors for PPROM include: previous PPROM, genital tract infections, antepartum bleeding, and cigarette smoking
-Presentation of rupture of membranes in a sudden gush of clear or pale yellow fluid leaking from the vagina.
-Physical exam may reveal amniotic fluid coming out of the cervical os or pooling in the vaginal fornix. This can be accentuated with coughing, valsalva or pushing on the fundus of the uterus
-Most women with PPROM will have low amount of amniotic fluid on ultrasound
-The majority of women with PPROM delivery within 1 week
-Nitrazine and Fern tests can help on physical exam if PPROM is not obvious on diagnosis. It assesses the pH. Amniotic fluid is usually 7.0-7.3, and the pH of the vagina is 3.8-4.2
-Patients that are 23-34 weeks with PPROM should be given a dose of corticosteroids to help mature the lungs.
-Corticosteroids has also been shown to reduce neonatal death, respiratory distress syndrome, intraventricular hemorrhage, and necrotizing enterocolitis
-Antibiotics are indicated to prolong latency and reduce the risk of neonatal group B streptococcal infection. Ampicillin 2 grams Q6 IV is recommended for 48 hours
-Tococlytics are used to delay delivery for 48 hours to give the steroids a chance to work
-Magnesium sulfate is administered prior to delivery for fetal neural protection
-In the absence of any contraindication to vaginal delivery, patients may proceed with a vaginal delivery after appropriate therapeutic measures are taken
-Rh Incompatibility-

-Rh negative women who deliver an Rh positive bay or who are otherwise exposed to Rh positive RBC are at risk of developing anti Rh antibodies
-Rh positive fetuses of these mothers are at risk of developing hemolytic disease of the fetus and newborn
-Rhogam, Rh (D) immunoglobulin, prophylaxis has led to a significant reduction in the frequency of maternal Rh alloimmunization, and associated neonatal complications
-Indications for Rhogam administration in an Rh negative mother
1. At approximately 28 weeks gestation
2. Within 3 days of delivery of an Rh positive infant
3. At the time of amniocentesis
4. After positive Kleihauer Betke test
5. After an ectopic pregnancy
6. After a spontaneous or induced abortion


















.jpg)
